When my daughter Rebekah took a job as the girls’ varsity basketball coach for the Lyle-Austin Pacelli Athletics, she prevailed upon me to be her assistant (and JV coach), so since mid-November we’ve been having a lot of time together.
We’ve lost a lot more games than we’ve won this season, but last night we achieved our first winning streak, following Tuesday night’s win with a big comeback against the Schaeffer Academy Lions. After being down 30-15 at halftime, the Athletics girls went on a 25-1 run to start the second half.
That was fun!
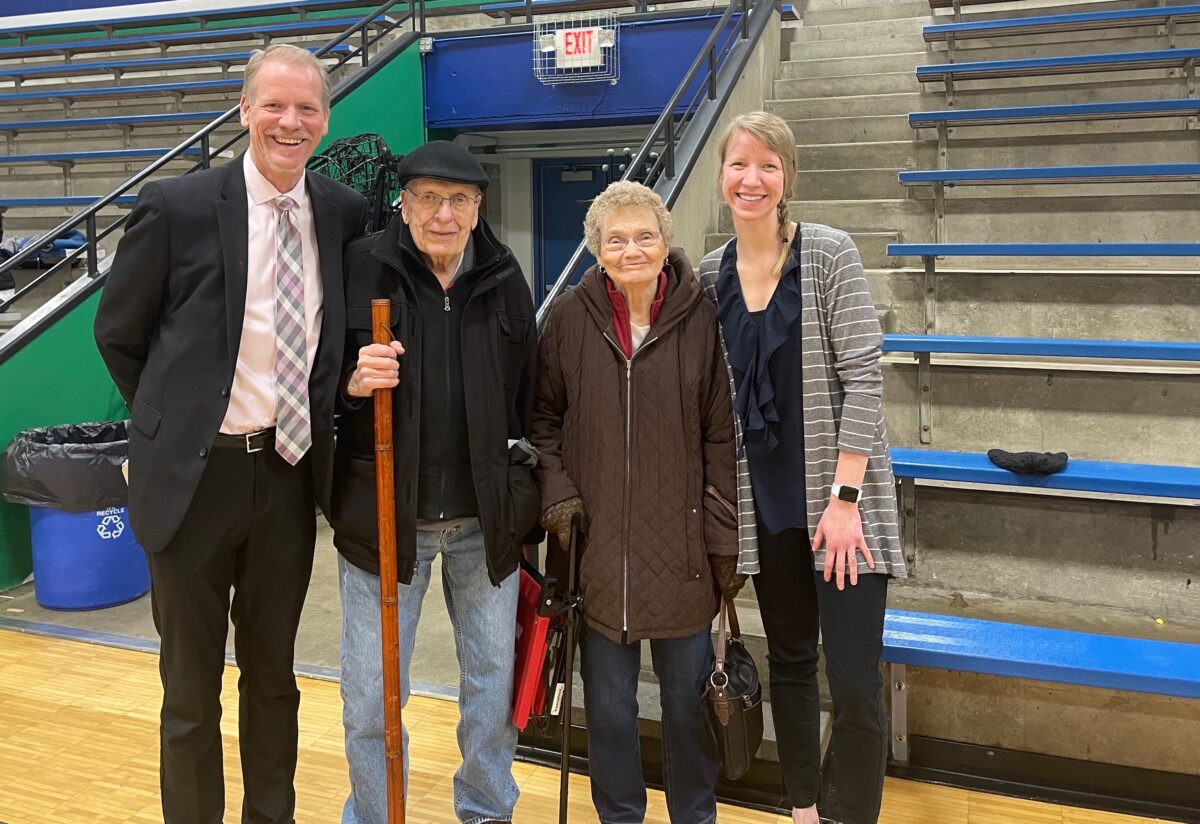
Afterward, Bekah and I took a picture with my parents, Lew and LaVonne, who were there to watch their son and granddaughter coach a great-granddaughter.

The basketball season will be wrapping up in the next couple of weeks, so then I will be focusing on another type of coaching Lisa and I are doing as part of our new venture, HELPcare.
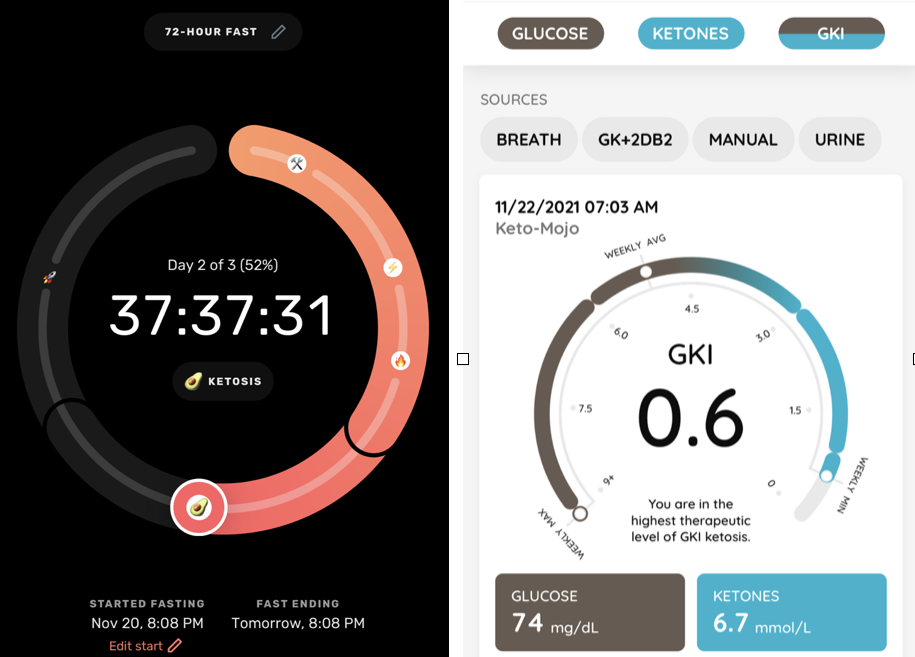
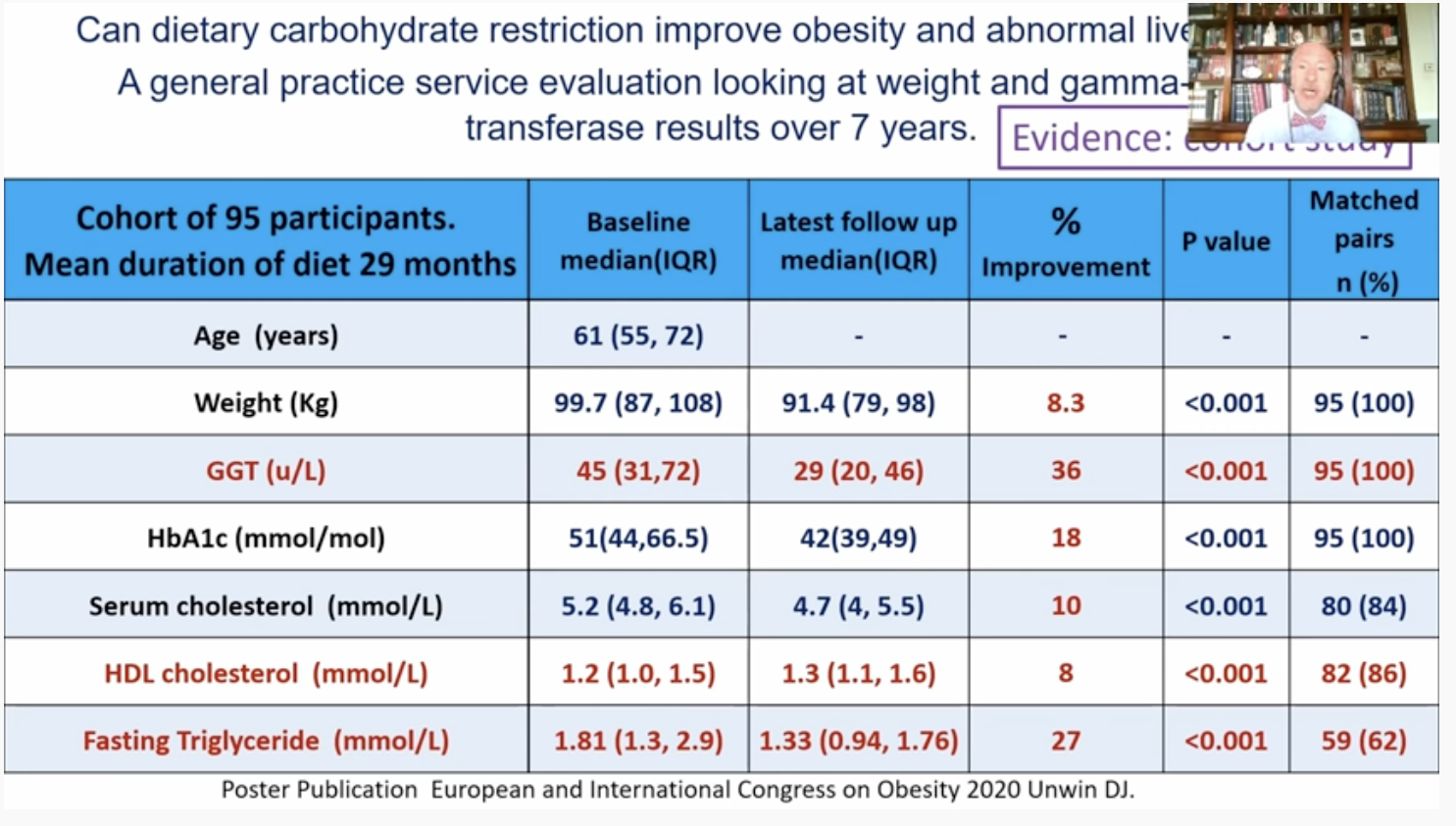
Through HELPcare we’re providing online education, community support and metabolic health coaching for people interested in making lifestyle changes to maximize their health, energy and longevity.
These services are available globally, but for people who become members of HELPcare Clinic they’re included at no extra charge.
HELPcare Clinic is the new direct primary care clinic I’m helping my good friend, Dr. David Strobel, open in our hometown of Austin, Minnesota. My new venture, HELPcare LLC, is contracted with HELPcare Clinic, his medical practice, to provide management services so he can focus on doctoring. We just opened last week.
This metabolic health coaching practice is built on what I’ve learned through my health journey over the last few years, and also the results Lisa has gotten. We started by coaching friends, and then the circle expanded over time.
I enjoy helping people discover their abilities to do more than they thought they could. It’s been really rewarding seeing people reclaim their health and even turn back the clock.
We feel better than we did 25 years ago, and are glad to help others looking to make similar changes.
And hopefully tonight we can make it three in a row for the Lyle-Pacelli girls!