While extended fasting can have a broad range of benefits, the real reason for my monthly three-day fast is for cancer prevention.
Professor Thomas Seyfried of Boston College, one of my Health Sherpas, has pioneered research that has significantly challenged the somatic mutation theory of cancer, which holds that cancer results from an accumulation of random DNA mutations in the nuclei of cells, which cause them to grow out of control.
Seyfried has championed a metabolic theory of cancer, which essentially says that cancer results from damaged mitochondria, the power plants of the cell.
The video below, in which he addresses a lay audience, provides a compelling presentation of his case.
He first dismantles the somatic mutation theory by showing how it is incompatible with the results of several studies.
He then convincingly describes the metabolic theory of cancer and how it better fits the data, explaining how cancer cells can have so many different mutations in the nuclear DNA, and yet have so many features in common.
The damaged mitochondria generate reactive oxygen species (ROS) that cause the DNA mutations in the cell nucleus. Those mutations are downstream from the real cause of cancers.
This video from last September is more technical, but also includes some updates on applications of his theory in cancer treatment. It’s worth watching if you want a deeper investigation.
Watch the video below first for an introduction, and afterwards scroll down and I’ll describe why I see a monthly three-day fast as a valuable cancer-prevention strategy.
You did watch it, right?
If not, hit the play button and read on when you’re done.
As Professor Seyfried explains, cancer cells use fermentation of sugar to generate energy, and lack the flexibility to use oxygen and ketones because of damaged mitochondrial structures.
As I mentioned previously, one of the benefits of fasting is autophagy, which causes cellular cleanup and recycling of defective organelles like the mitochondria. So one cancer-prevention mechanism is replacing mitochondria that are throwing off ROS and causing mutations with new and improved versions.
The second mechanism is by introducing ketosis at a level that is far beyond a typical ketogenic diet. We all have lots of cancer cells in our bodies at any given time, and our immune system kills off many of them.
But as Professor Seyfried says, cancer cells have lost the metabolic flexibility to use ketones for energy because of their damaged mitochondria. An extended fast drives ketone levels high enough to cause the remaining cancer cells to die, or at least slows their ability to grow and proliferate.
Ketones and blood sugar are inversely related. As blood sugar goes down due to caloric restriction (or a fast), ketone levels go up. And as glucose goes up, tumor size increases.
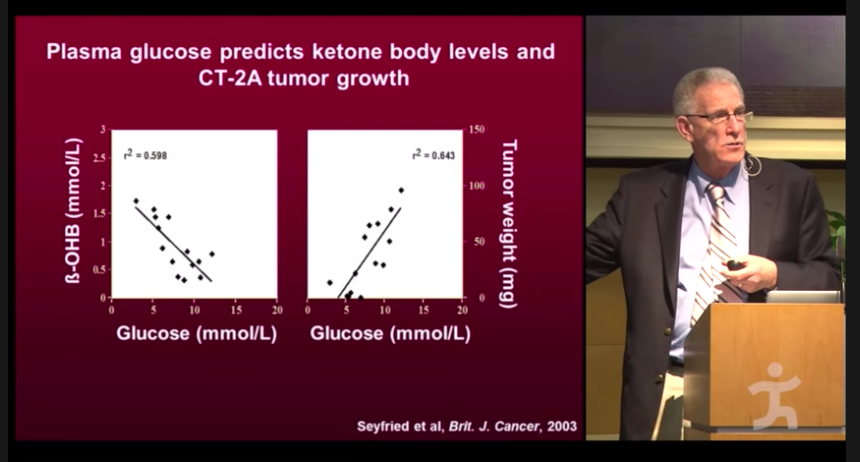
“It doesn’t mean that sugar causes the cancer, but if you have the tumor, the tumor will grow faster with the higher blood sugar.”
Professor Thomas Seyfried
Later in the video, in the Q&A session, Professor Seyfried describes meeting members of the Calorie Restriction Society of America, people who severely and continuously limit their food intake, and how they have virtually zero incidence of cancer.
He also suggests that long-term caloric restriction is no way to live.
I agree with that.
I see periodic episodes of extended fasting as a way of getting most of the benefits of long-term caloric restriction without the soul-crushing grind of continual deprivation.
As I said in my last post, no one really knows how long is long enough for these extended fasts, or how frequently they should be done.
In my next post I’ll describe why I’ve settled on a three-day fast once a month as my dosage, with a low-carb, high fat (LCHF) lifestyle and time-restricted feeding as the foundation.
If you think your friends might find this post helpful, I hope you’ll share by email or on your social networks using the buttons below.
To get these updates on a regular basis you can subscribe by email, or follow me on Facebook, Twitter and LinkedIn, where I’ll also be posting links.
Check out My Health Journey for the full story of our health improvements, and my #BodyBabySteps for an approach to how I would do it if I were starting today, based on what I’ve learned.
